All published articles of this journal are available on ScienceDirect.

Smartphone Addiction among University Students
Authors Info & Affiliations
Abstract
Introduction
Excessive smartphone usage has raised concerns about addiction and its potential detrimental effects on students' mental health and academic performance.
Methods
A cross-sectional study was conducted among 343 nursing, physiotherapy, and midwifery students at the University of Shkodra using a 10-item online questionnaire to assess smartphone use, dependence, and related behaviors. Data were collected in January and February 2025. Analyses included exploratory factor analysis and hierarchical OLS regression using SPSS 19.
Results
All students reported using smartphones; 48.1% used their phones for 4–6 hours daily, consistent with global trends of increasing smartphone addiction. About 50.4% used smartphones primarily for social media, research, news, and entertainment. A strong emotional attachment was evident, with 84.6% experiencing anxiety or distress when without their phones. Physical symptoms were also reported, with 23% experiencing wrist or neck pain due to prolonged use, underscoring the importance of ergonomic awareness.
Discussion
The findings reflect global trends in student smartphone overuse, with emotional dependence and physical strain being the most prominent concerns. In Albania, limited student support and digital literacy may intensify reliance on smartphones as coping tools, highlighting the need for targeted interventions.
Conclusions
Students at the University of Shkodra exhibit growing smartphone dependence that affects their daily life and well-being. Both mental distress and physical discomfort highlight potential health risks linked to smartphone addiction.
1. INTRODUCTION
Smartphones are an integral part of daily life, particularly for university students who rely on them for academic work, social interactions, and entertainment. However, excessive smartphone usage has raised concerns about addiction and its potential detrimental effects on students' mental health and academic performance. Smartphone addiction is increasingly recognized as a global issue, with studies from various countries highlighting its prevalence among young people and its negative impact on cognitive functions, mental well-being, and academic outcomes [1, 2].
A systematic review demonstrated that smartphone addiction among nursing students is linked to stress, anxiety, and burnout, adversely affecting their academic performance and overall well-being [3]. Moreover, smartphone addiction is often associated with poor sleep quality, which further exacerbates academic challenges [4]. Excessive smartphone use has been associated with numerous mental health problems, such as elevated stress levels, anxiety, and depression. The constant connectivity and exposure to social media can lead to feelings of isolation and negatively impact students' well-being [5].
The widespread use of smartphones has been linked to a decline in face-to-face social interactions. Students may become more engaged in their devices than in in-person communications, leading to potential declines in social skills and increased feelings of loneliness [6].
International research has also highlighted that smartphone use patterns among students are significantly influenced by social, cultural, and academic contexts, with a direct impact on students' daily lives and overall productivity. For instance, studies in South Korea and China revealed that excessive smartphone use was linked to reduced academic performance, lower attention spans, and poor academic engagement [7, 8]. In contrast, research from Western countries, such as the United States and the United Kingdom, has demonstrated that smartphone addiction leads to increased stress levels, depression, and a sense of isolation among students [9, 10].
Moreover, the rise of social media platforms and their integration with smartphones has further contributed to the addictive use of these devices. Social media apps, including Facebook, Instagram, and TikTok, are designed to be highly engaging, which has led to prolonged use among students. A study on Fear of Missing Out (FOMO) [11] in Europe highlighted that social media addiction negatively affects students' ability to concentrate and contributes to academic procrastination [12]. Additionally, smartphone addiction has been found to contribute to the development of mental health problems such as anxiety, depression, and self-esteem issues, particularly among young adults [13]. In Albania, the issue of smartphone addiction among students has gained attention in recent years, leading to government action, such as the ban on TikTok in 2025 due to concerns over its impact on the behavior of youth [14]. Albanian studies have also identified significant negative effects of smartphone use on students' academic performance and mental health [15]. Studies observed that excessive smartphone use among Albanian students negatively influenced their academic focus and study habits. At the same time, they found that smartphone addiction was linked to increased levels of stress and anxiety among students [16, 17].
Given the growing concerns about smartphone addiction, this study aims to examine its prevalence and dimensions. We focused on nursing, physiotherapy, and midwifery students at the University of Shkodra. Specifically, the research investigated how different forms of dependence — emotional, habitual, and strain-related —are associated with daily smartphone use, and how behavioral and emotional responses (such as nighttime phone checking and anxiety when separated from the phone) may influence or moderate this relationship. By identifying key psychological and usage-related predictors of smartphone dependence, the study seeks to contribute to the development of evidence-based strategies to promote responsible smartphone use and support student well-being in academic environments.
2. MATERIALS and METHODS
2.1. Theoretical Framework and Hypotheses
This study draws on several theoretical models to provide a comprehensive understanding of smartphone dependence among university students. The primary framework employed is the I-PACE model (Interaction of Person–Affect–Cognition–Execution), which conceptualizes technology-related addictive behaviors as arising from the interaction of personal characteristics (e.g., impulsivity, emotional vulnerability), affective and cognitive responses (e.g., anxiety, compulsive checking), and situational factors (e.g., device accessibility, social context) [18]. Within this framework, smartphone dependence is viewed not as a unidimensional construct but as a multidimensional process shaped by emotional, habitual, and awareness-related factors.
To complement this perspective, the study also draws upon the Uses and Gratifications Theory (UGT), which posits that individuals actively use media to satisfy personal needs, such as emotional regulation, social connection, and entertainment [19, 20]. UGT helps explain the motivational drivers behind smartphone overuse, especially in academic settings where students may use their devices to manage stress or avoid academic pressure. Furthermore, the Compensatory Internet Use Theory (CIUT) supports the notion that excessive smartphone use may function as a coping mechanism for underlying psychological distress, such as anxiety or loneliness, which may be particularly prevalent in the student population [21].
Based on these theoretical foundations, the study investigates how different dimensions of smartphone dependence—namely, emotional/habitual and strain-related awareness relate to daily smartphone use. It also examines how behavioral indicators (e.g., nighttime phone checking) and emotional responses (e.g., anxiety when separated from the phone) not only predict usage but may also moderate the relationship between dependence and usage intensity. Finally, demographic and academic characteristics such as age, gender, and year of study are included as control variables, as prior literature suggests that their influence on smartphone use may be inconsistent or weak.
To empirically test these theoretical assumptions, the following hypotheses were developed:
H1. All other things being equal, higher levels of smartphone dependence will be positively associated with the duration of daily smartphone use. (I-PACE Model)
- H1a. All other things being equal, emotional/habitual dependence will be positively related to estimated daily smartphone use.
- H1b. All other things being equal, strain/external awareness dependence will be positively related to estimated daily smartphone use.
H2. All other things being equal, specific smartphone-related behaviors and emotional reactions will predict higher levels of smartphone use. (I-PACE Model; CIUT)
- H2a. All other things being equal, individuals who check their phones at night will report higher daily smartphone use.
- H2b. All other things being equal, individuals who experience anxiety when forgetting their phone will report higher daily smartphone use.
H3. All other things being equal, the relationship between smartphone dependence and daily smartphone use will be moderated by behavioral and emotional responses to phone use. (I-PACE Model)
- H3a. All other things being equal, the positive association between emotional dependence and smartphone use will be stronger among those who report anxiety when forgetting their phone.
- H3b. All other things being equal, the positive association between strain dependence and smartphone use will be stronger among those who check their phone at night.
H4. All other things being equal, sociodemographic characteristics, such as age, gender, and academic year, will exhibit weak or inconsistent associations with daily smartphone use. (UGT)
2.2. Model Estimation Strategy
We test the hypotheses using hierarchical linear regression models applied to cross-sectional survey data from 343 students. The unit of analysis is the individual student. The primary dependent variable, estimated daily smartphone use (in hours), is treated as a continuous variable and regressed on a set of individual-level psychological, behavioral, and demographic predictors.
All models are estimated using Ordinary Least Squares (OLS) regression with listwise deletion for missing values. We proceed in stages, incrementally adding theoretically relevant blocks of predictors to assess improvements in model fit and explanatory power. Robust standard errors are used in all models to account for potential heteroskedasticity.
2.3. Methodology
2.3.1. Participants and Data Collection
Data for this study were collected between January and February 2025 using a structured, self-administered questionnaire designed to assess patterns of smartphone use, dependence, and associated psychological and behavioral factors. From a total of 700 bachelor students enrolled in Nursing, Midwifery, and Physiotherapy programs at the Faculty of Health Sciences, University of Shkodra “Luigj Gurakuqi”, 343 students participated in this study (Fig. 1). A minimum sample size of 249 participants was calculated to ensure a 95% confidence level with a ±5% margin of error, indicating that the achieved sample size exceeds the minimum requirement for robust analysis.
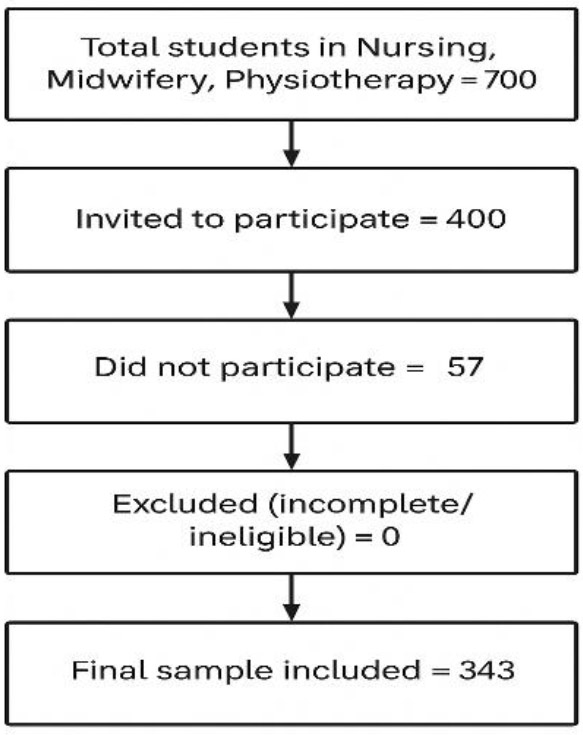
Participant selection process.
A purposive sampling strategy was employed to ensure balanced representation across the three main academic disciplines within the faculty: Nursing, Midwifery, and Physiotherapy. This approach was selected to allow for targeted exploration of smartphone use within student populations most relevant to the study’s objectives. All Bachelor students actively enrolled in these programs during the study period were invited to participate either via online links distributed through institutional channels or in classroom sessions under faculty supervision. Additionally, to enhance accessibility and participation rates, the survey link was shared via official WhatsApp academic groups used for student communication. This mixed-mode approach helped reach students more effectively while minimizing potential selection bias related to digital access or availability. Participation was entirely voluntary, and informed consent was obtained from all participants prior to data collection. Before completing the questionnaire, students were presented with an introductory information section that explained the study’s purpose, the voluntary nature of participation, their right to withdraw at any time without consequence, and the procedures in place to ensure anonymity and confidentiality. No personally identifying information was collected, and all responses were stored securely in password-protected files accessible only to the research team. Responses that were incomplete or submitted by students outside the target fields were excluded to preserve data integrity. The sample was predominantly female (90.7%), reflecting the gender distribution in health-related fields, with participant ages ranging from 18 to 38 years (M = 20.27, SD = 2.44). While the sample’s gender imbalance may limit broader generalizability, it accurately represents the target population within these disciplines.
2.3.2. Inclusion and Exclusion Criteria
Participants were selected based on predefined inclusion and exclusion criteria to ensure relevance and data integrity. Eligible individuals included undergraduate students enrolled in the Nursing, Midwifery, or Physiotherapy programs at the Faculty of Health Sciences, University of Shkodra “Luigj Gurakuqi,” during the 2024–2025 academic year. The inclusion criteria required participants to be at least 18 years of age and to be active smartphone users, ensuring adequate exposure to digital technologies relevant to the study's objectives. Informed consent was obtained from all participants following a detailed explanation of the study’s purpose, procedures, voluntary nature, and measures taken to ensure anonymity and confidentiality.
Students who were not enrolled in the target programs, not active during the data collection period, or who submitted incomplete or invalid responses were excluded from the analysis. These selection parameters were implemented to enhance the representativeness and quality of the data collected.
2.4. Measures
2.4.1. Dependent Variable
2.4.1.1. Estimated Daily Smartphone Use
The primary outcome variable is the self-reported average number of hours participants use their smartphones each day, excluding voice calls. Participants responded to a categorical item with time ranges (e.g., “1–3 hours,” “4–6 hours”), which were subsequently recoded into a continuous scale from 0.5 to 10 hours based on the midpoints of the categories. This measure captures daily exposure and engagement with smartphones in non-communicative functions, aligning with behavioral dependence literature.
2.4.2. Independent Variables
2.4.2.1. Smartphone Dependence Scale
A composite measure of smartphone dependence was constructed using 10 items adapted from validated scales assessing problematic use and digital attachment. Items reflected emotional, behavioral, and physical dimensions of dependence (e.g., “You feel anxious when you forget your phone,” “You use your phone longer than you intended”). Responses were rated on a 6-point Likert scale (1 = Strongly Disagree to 6 = Strongly Agree). Exploratory factor analysis using principal component analysis with varimax rotation revealed a two-factor solution: (i) Emotional/Habitual Dependence: Reflecting compulsive checking, emotional reliance, and habit-driven use. (ii) Strain/External Awareness: Capturing awareness of overuse and its consequences, such as concentration difficulties and physical discomfort. Factor scores for both components were computed and used as continuous predictors in the regression models. The Emotional/Habitual Dependence factor demonstrated excellent internal consistency, with a Cronbach’s alpha of .844. Consistently, the Strain/External Awareness factor showed good internal consistency (α = .801), supporting the reliability of both dimensions derived from the scale.
2.5. Phone Anxiety
This variable reflects whether participants experience anxiety when separated from their smartphones. It was operationalized as a binary variable, coded 1 if participants agreed with the statement “You feel anxious when you forget your phone,” and 0 otherwise.
2.6. Nighttime Checking Behavior
To measure nocturnal attachment to smartphones, participants were asked whether they check their phones during nighttime awakenings. Responses were coded as a binary variable (1 = Yes, 0 = No).
2.7. Control Variables
Demographic and academic background characteristics were included as controls to isolate the effects of psychological predictors:
- Age was included as a continuous variable, along with Age Squared (Age2), to capture potential curvilinear relationships between age and smartphone use.
- Gender was coded 1 for female and 0 for male participants.
- Urban Residence was coded 1 for participants residing in urban areas and 0 for those in rural areas.
- The field of study was captured through dummy variables for the Physiotherapy, Nursing, and Midwifery tracks, with the latter serving as the reference group.
- The year of study was measured using dummy variables for each academic year in the bachelor's cycle (Year 1, Year 2, Year 3). The master's program was excluded from the analysis due to the absence of observed variation.
2.8. Analytical Strategy
To test the study's hypotheses, a hierarchical regression modeling approach was employed using Ordinary Least Squares (OLS) estimation. This strategy enables the incremental examination of how demographic, behavioral, and psychological variables contribute to variation in daily smartphone use. Models were built in successive steps: Model 1 included only demographic and educational controls (age, gender, urban residence, study field, and year). Model 2 added the behavioral variable for nighttime checking, and Model 3 introduced phone-related anxiety. In the final step (Model 4), the two latent dimensions of smartphone dependence, emotional/habitual and strain/external awareness, were added to assess their unique explanatory power.
To further explore conditional effects, interaction terms were introduced in subsequent models (Model 5a–5d) to test whether the effects of emotional and strain-based dependence were moderated by phone anxiety and nighttime checking behaviors. All continuous variables were mean-centered prior to constructing interaction terms to reduce multicollinearity and ease interpretability [22]. Variance inflation factors (VIFs) were examined across all models and confirmed that multicollinearity was not a concern. All models were estimated using OLS regression with listwise deletion applied for missing data to ensure model consistency and comparability across steps.
3. RESULTS
3.1. Descriptive Statistics
From a total of 700 bachelor students enrolled in Nursing, Midwifery, and Physiotherapy programs, 400 students were invited to participate in the study. Among these, 57 students declined to participate or did not respond, resulting in 343 students completing the questionnaire and being included in the final analysis (Fig. 1). This response rate is in line with participation trends in cross-sectional studies on smartphone use among health sciences students [1, 3]. Table 1 presents descriptive statistics for the key variables included in the analysis. The sample consists of 343 university students with a mean age of 20.27 years (SD = 2.44), ranging from 18 to 38 years. The squared age variable (M= 416.87, SD = 120.30) was included to account for potential nonlinear effects in the relationship between age and smartphone dependence, in line with previous studies that employed similar modeling approaches [2]. Among the 343 participants, 90.7% (n = 311) were female and 9.3% (n = 32) were male. This gender distribution (M = 0.91, SD = 0.29) reflects the predominance of females in nursing and midwifery programs and aligns with prior research [23].
Approximately half of the participants reported residing in urban areas (M = 0.53, SD = 0.50), indicating a balanced distribution between urban and rural origins.
In terms of academic background, the majority of students were enrolled in the Nursing program (M = 0.73), followed by Midwifery (M = 0.22), and a smaller share in Physiotherapy (M = 0.05). These distributions are consistent with enrollment trends in similar higher education contexts in the Western Balkans [15, 16]. The master's program was not represented in the dataset, as indicated by a mean of 0.00. Regarding academic year, students were fairly evenly distributed across the three bachelor cohorts: Year 1 (M = 0.27), Year 2 (M = 0.39), and Year 3 (M = 0.27).
| Variable | N | Min | Max | M | SD |
|---|---|---|---|---|---|
| Age | 343 | 18.00 | 38.00 | 20.27 | 2.44 |
| Age Squared (Age2) | 343 | 324.00 | 1444.00 | 416.87 | 120.30 |
| Female (1 = Female, 0 = Male) | 343 | 0.00 | 1.00 | 0.91 | 0.29 |
| Urban Residence (1 = Urban, 0 = Rural) | 343 | 0.00 | 1.00 | 0.53 | 0.50 |
| Study Cycle: Physiotherapy | 343 | 0.00 | 1.00 | 0.05 | 0.22 |
| Study Cycle: Nursing | 343 | 0.00 | 1.00 | 0.73 | 0.45 |
| Study Cycle: Midwifery | 343 | 0.00 | 1.00 | 0.22 | 0.41 |
| Study Year: Bachelor Year 1 | 343 | 0.00 | 1.00 | 0.27 | 0.45 |
| Study Year: Bachelor Year 2 | 343 | 0.00 | 1.00 | 0.39 | 0.49 |
| Study Year: Bachelor Year 3 | 343 | 0.00 | 1.00 | 0.27 | 0.45 |
| Has Smartphone | 343 | 0.00 | 1.00 | 0.99 | 0.09 |
| Daily Use: <1 hour | 343 | 0.00 | 1.00 | 0.02 | 0.14 |
| Daily Use: 1–3 hours | 343 | 0.00 | 1.00 | 0.32 | 0.47 |
| Daily Use: 4–6 hours | 343 | 0.00 | 1.00 | 0.48 | 0.50 |
| Daily Use: 7–9 hours | 343 | 0.00 | 1.00 | 0.12 | 0.32 |
| Daily Use: >9 hours | 343 | 0.00 | 1.00 | 0.06 | 0.23 |
| Estimated Smartphone Use (hours/day) | 343 | 0.50 | 10.00 | 4.60 | 2.38 |
| Checks Phone at Night (1 = Yes) | 343 | 0.00 | 1.00 | 0.49 | 0.50 |
| Anxious Without Phone (1 = Yes) | 343 | 0.00 | 1.00 | 0.85 | 0.36 |
| Total Smartphone Dependence Score (10–60) | 343 | 10.00 | 59.00 | 33.94 | 9.30 |
| Average Smartphone Dependence Score (1–6) | 343 | 1.00 | 5.90 | 3.39 | 0.93 |
| Dependence – Emotional/Habitual (Factor 1) | 343 | 1.00 | 6.00 | 3.44 | 1.12 |
| Dependence – Strain/External Awareness (Factor 2) | 343 | 1.00 | 6.00 | 3.35 | 0.97 |
Virtually all respondents reported owning a smartphone (M = 0.99, SD = 0.09), suggesting that mobile technology use is pervasive among this population and consistent with global patterns [4, 5]. Regarding daily smartphone use, the average estimated usage was 4.60 hours per day (SD = 2.38), with usage ranging from a minimum of 30 minutes to a maximum of 10 hours. Most students reported using their phones between 4 and 6 hours per day (48%), followed by 1–3 hours (32%). This pattern mirrors findings from prior studies among university students, indicating that 4–6 hours of daily smartphone use is the most common range [1, 6, 24].
A smaller portion reported higher usage: 7–9 hours (12%) and more than 9 hours (6%). Only 2% reported using their phones for less than an hour daily (Table 1).
Notably, 49% of participants admitted to checking their phone when they wake up at night, indicating the habitual and potentially compulsive nature of smartphone engagement behavior documented as a marker of problematic use in previous studies [7, 10]. Furthermore, a striking 85% of students reported experiencing anxiety when separated from their smartphone, an indicator of psychological dependence, which is widely recognized in the literature [11, 17]. The total smartphone dependence score ranged from 10 to 59 (out of a possible 60), with a mean of 33.94 (SD = 9.30). The average item score was 3.39 (SD = 0.93) on a 6-point Likert scale, reflecting moderate levels of perceived dependence. These results are comparable to those obtained in studies utilizing the Smartphone Addiction Scale-Short Version (SAS-SV) [2, 25]. When examining the two sub-dimensions derived from factor analysis, the mean score for Emotional/Habitual Dependence was 3.44 (SD = 1.12), while Strain/External Awareness scored slightly lower at 3.35 (SD = 0.97). These findings suggest that emotional attachment and habitual use may be more prominent drivers of dependence than physical discomfort or awareness of overuse [13, 18, 26].
Together, the descriptive results provide an initial overview of the demographic composition, usage patterns, and psychological indicators of smartphone dependence among health sciences students. The high prevalence of usage and psychological attachment warrants further investigation through multivariate modeling, presented in the sections that follow.
3.2. Factor Structure of Smartphone Dependence
Exploratory factor analysis using principal component analysis with Varimax rotation revealed a two-factor structure underlying the 10-item Smartphone Dependence Scale. This dimensionality aligns with previous studies that support the multidimensional nature of problematic smartphone use, particularly in academic populations [2, 3, 13].
The first factor, Emotional/Habitual Dependence, accounted for the highest loadings on items reflecting compulsive or emotionally driven behaviors, such as “Feels impatient when not holding phone” (0.790), “Can’t be without smartphone” (0.736), and “Thinks about smartphone even when not using it” (0.698) (Table 2).
This factor captures the affective and routine-driven aspects of smartphone engagement, reflecting internalized behavioral patterns, such as emotional regulation through device use or habitual checking behaviors [7, 18].
The second factor, Strain/External Awareness, captured items that reflect psychological strain or physical discomfort related to phone use, such as “Feels anxious when phone is forgotten” (0.773), “Difficulty concentrating due to phone use” (0.650), and “Pain in hands or neck from smartphone use” (0.640) (Table 2). This dimension is similar to those found in other studies that differentiate between internal dependency and externalized consequences of use [26, 27]. This factor represents the tension and external pressure individuals may feel in response to their smartphone habits. Several items demonstrated meaningful cross-loadings, such as “Uses phone longer than intended” (0.452 on Factor 1 and 0.590 on Factor 2), indicating overlap between emotional compulsion and perceived strain, an overlap also identified in previous research on problematic smartphone use among students [1, 25]. However, the factor structure clearly distinguishes between emotionally driven dependence and the strain or awareness of overuse, supporting the multidimensional nature of smartphone dependence among students. These findings provide strong construct validity for using the two sub-dimensions, Emotional/Habitual and Strain/External Awareness, in subsequent regression analyses and are consistent with the literature on digital behavior modeling among university students [13, 18].
| Item | Factor 1 Emotional/ Habitual) |
Factor 2 (Strain/External Awareness) |
|---|---|---|
| Can’t be without a smartphone | 0.736 | 0.019 |
| Feels impatient when not holding the phone | 0.790 | 0.229 |
| Thinks about the smartphone even when not using it | 0.698 | 0.389 |
| Believes life depends on smartphone use | 0.692 | 0.226 |
| Checks phone to avoid missing social media | 0.641 | 0.237 |
| Feels anxious when the phone is forgotten | 0.079 | 0.773 |
| Difficulty concentrating due to phone use | 0.219 | 0.650 |
| Pain in the hands or neck from smartphone use | 0.106 | 0.640 |
| Uses the phone longer than intended | 0.452 | 0.590 |
| Others say the phone is overused | 0.366 | 0.588 |
3.3. Bivariate Correlations
Table 3 presents Pearson correlations among the study’s key variables. As expected, age and age squared are highly correlated (r = 0.992, p < 0.001), which is typical due to the mathematical relationship between the two variables. Age was negatively associated with both smartphone use (r = –0.113, p < 0.05) and smartphone dependence scores (r = –0.100 to –0.111, p < 0.05), indicating that younger students report slightly higher use and dependence. This inverse association has also been reported in previous studies that emphasize increased vulnerability among younger users [1, 26].
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Age | — | - | - | - | - | - | - | - | - |
| 2. Age2 | 0.992** | — | - | - | - | - | - | - | - |
| 3. Female (1 = Yes) | 0.003 | 0.011 | — | - | - | - | - | - | - |
| 4. Urban (1 = Urban) | 0.092 | 0.089 | -0.099 | — | - | - | - | - | - |
| 5. Smartphone Use (hours/day) | -0.113* | -0.113* | 0.038 | 0.018 | — | - | - | - | - |
| 6. Night Check (1 = Yes) |
-0.034 | -0.042 | -0.008 | -0.048 | 0.228** | — | - | - | - |
| 7. Phone Anxiety (1 = Yes) |
-0.101 | -0.103 | 0.002 | -0.076 | 0.117* | 0.303** | — | - | - |
| 8. Smartphone Dependence (Average Score) |
-0.100 | -0.113* | -0.011 | -0.093 | 0.439** | 0.278** | 0.366** | — | - |
| 9. Emotional Dependence (Factor 1) |
-0.111* | -0.131* | -0.031 | -0.067 | 0.368** | 0.282** | 0.393** | 0.906** | — |
| 10. Strain Dependence (Factor 2) |
-0.063 | -0.065 | 0.015 | -0.101 | 0.418** | 0.209** | 0.250** | 0.873** | 0.584** |
Gender was not significantly correlated with any of the primary outcomes, although females showed a small, non-significant tendency toward higher smartphone use and dependence. Urban residence similarly showed weak and non-significant associations, confirming previous findings that sociodemographic characteristics are often less predictive than psychological or behavioral factors [6, 24].
As hypothesized, estimated daily smartphone use was positively and moderately associated with average smartphone dependence (r = 0.439, p < 0.001), emotional dependence (r = 0.368, p < 0.001), and strain dependence (r = 0.418, p < 0.001). These findings are consistent with prior research showing that increased usage duration is a core indicator of digital dependence [2, 25].
Nighttime checking behavior was significantly associated with higher smartphone use (r = 0.228, p < 0.001) and with both emotional (r = 0.282, p < 0.001) and strain-related dependence (r = 0.209, p < 0.001), reflecting habitual and potentially compulsive behavior patterns [10, 17]. Phone anxiety, the self-reported feeling of distress when forgetting the smartphone, was positively associated with all smartphone dependence measures (r = 0.366 to 0.393, all p < 0.001), supporting previous research on nomophobia and its link to excessive use [11, 18] (Table 3).
The two dependence subscales, Emotional/Habitual and Strain/External Awareness, were strongly correlated (r = 0.584, p < 0.001), suggesting related but distinct dimensions. This justifies their use as separate predictors in multivariate modeling [13, 27]. These correlations provide preliminary support for the study’s hypotheses regarding the psychological and behavioral dimensions of smartphone overuse.
Table 4 presents the results of hierarchical OLS regression models predicting average smartphone dependence, measured on a 6-point Likert scale. The models assess the incremental explanatory power of sociodemographic characteristics and key behavioral predictors.
Model 1 included age, age squared, gender (female), and urban residence. This baseline specification explains a small but statistically significant portion of variance in smartphone dependence (R2 = 0.030, p < 0.05). Age shows a curvilinear effect: while age is positively associated with smartphone dependence (b = 0.304, p = 0.066), the squared age term is negatively associated (b = -0.007, p = 0.039), indicating diminishing returns or a plateauing of dependence with increasing age. Female gender and urban residence do not significantly predict dependence scores in this baseline model (Table 4).
Model 2 introduced estimated daily smartphone use, which substantially improved the model fit (R2 = 0.218, Adjusted R2 = 0.206, p < 0.001). Smartphone use emerged as a strong and significant predictor of dependence (b = 0.171, SE = 0.019, p < 0.001), confirming that duration of use is closely tied to problematic engagement [25]. Age remained significant in this model, while sociodemographic predictors stayed non-significant (Table 4).
Model 3 added two psychological variables, phone anxiety and nighttime checking, which increased the explained variance to 31.9% (R2 = 0.319, Adjusted R2 = 0.304, p < 0.001). Phone anxiety was the strongest predictor (b = 0.728, p < 0.001), while nighttime checking was marginally significant (b = 0.174, p = 0.054) (Table 4). These findings reinforce the role of emotional responses in driving excessive smartphone use [11, 18, 21].
Notably, the effect of daily use remained robust (b = 0.150, p < 0.001) even after controlling for psychological variables (Table 4). These results confirm prior evidence that behavioral and emotional factors, rather than demographic characteristics, are more predictive of smartphone overuse [20, 25].
Across all three models, the final specification demonstrated that frequent usage, psychological anxiety, and nighttime checking are independently associated with greater dependence, even when age, gender, and location are controlled. Age maintained a consistent curvilinear effect throughout, but with relatively modest influence. Moreover, interpreting the unstandardized coefficients provides practical implications. The coefficient for phone anxiety (b = 0.728) suggests that students who report such anxiety use their phones for approximately 43 minutes more per day than those who do not. The coefficient for nighttime checking (b = 0.174) reflects an average increase of 10 minutes in daily use. These results emphasize the significant role of internal emotional drivers in predicting problematic smartphone behavior [13, 18].
| Predictor | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Phone Anxiety (1=yes) | - | - | 0.728 (0.123)*** |
| Night Check (1=yes) | - | - | 0.174 (0.090)* |
| Daily smartphone use | - | 0.171 (0.019)*** | 0.150 (0.018)*** |
| Urban (1=Urban) | -0.164 (0.101) | -0.191 (0.091)* | -0.143 (0.085) |
| Female (1=yes) | -0.038 (0.172) | -0.097 (0.155) | -0.084 (0.145) |
| Age | 0.304 (0.165) | 0.313 (0.148)* | 0.284 (0.139)* |
| Age2 | -0.007 (0.003)* | -0.007 (0.003)* | -0.006 (0.003)* |
| R2 | 0.030 | 0.218 | 0.319 |
| Adjusted R2 | 0.018 | 0.206 | 0.304 |
| F(df) | 2.585 (338)* | 81.043 (337)*** | 24.764 (335)*** |
| N | 342 | 342 | 342 |
| Constant | 0.244 (1.982) | -0.746 (1.786) | -1.124 (1.678) |
4. DISCUSSION
Our study on smartphone use among students at “Luigj Gurakuqi” University aligns with findings from similar research conducted in various regions.
The high percentage of students in our study reporting smartphone use (100%) and the significant daily usage times (48.1% use for 4-6 hours) aligns with other research on smartphone addiction among university students. A study among university students in Pakistan found that 62.1% of students spent over 4 hours a day on their smartphones [24]. Similarly, in our study, a large percentage of students (48.1%) reported using smartphones for 4-6 hours daily, indicating an increased risk of smartphone addiction due to prolonged usage.
Notably, a cross-sectional study among undergraduate medical students in Assam, India, reported a smartphone addiction prevalence of 44.07% [26]. Similarly, research involving freshmen medical students in China identified a smartphone addiction rate of 39.7% [23]. In the Assam study, higher daily smartphone usage was associated with increased addiction risk. Specifically, students using smartphones for 3-4 hours daily were 3.2 times more likely to be addicted, while those exceeding 5 hours daily had a 5.7 times higher risk. This correlation between usage duration and addiction risk aligns with our findings, where a substantial portion of students reported daily usage between 4-6 hours.
Furthermore, in our study, 50.4% of students reported using smartphones for multiple activities, such as social networking, research, news, and entertainment. This multifaceted use is consistent with global trends where smartphones serve as all-encompassing tools for both academic and social engagement. Another study provides evidence of similar patterns in students from various disciplines, with smartphones predominantly used for educational purposes, followed by social media and entertainment [25]. The widespread use of smartphones for academic-related tasks could indicate both positive and negative effects, as excessive use could disrupt sleep patterns and lead to symptoms of digital addiction.
Another significant finding from our study was the distress students felt when they forgot their phones elsewhere, with 84.6% reporting feelings of anxiety or distress. This finding is consistent with a study that noted anxiety about being without a smartphone as a common psychological response among university students in China [28]. The emotional attachment to smartphones observed in our study highlights the need for awareness and intervention to mitigate the mental health risks associated with excessive smartphone use.
Additionally, the impact of smartphone use on physical health was evident in our study, with 23% of students reporting wrist and neck pain due to prolonged usage. This finding is supported by other studies [27], which reported similar musculoskeletal discomfort among students who spent long hours on their smartphones. The physical repercussions of excessive smartphone use suggest the importance of addressing ergonomics and promoting healthier usage habits among students.
In conclusion, our findings emphasize the growing concern over smartphone addiction among university students. Similar to studies conducted globally, prolonged usage and emotional dependence on smartphones are associated with both physical and mental health challenges. It is crucial for universities to implement strategies to educate students on responsible smartphone use and the potential risks of excessive dependence. Further research should focus on interventions and preventive measures to reduce smartphone addiction and promote healthier digital habits among students.
While the prevalence of smartphone dependence in our sample reflects global patterns reported in studies from Asia and Europe, the underlying factors may differ significantly due to contextual influences. In contrast to highly digitalized societies where overuse may stem from constant work or academic surveillance, in the Albanian context, overuse may be partly driven by limited access to alternative recreational or academic outlets. University students in Albania often lack structured campus activities, extracurricular engagement, and accessible mental health services, which may increase reliance on smartphones as a coping mechanism [29].
Psychologically, smartphone use may serve as an emotional regulator in the face of academic stress and uncertainty, particularly in fields, such as nursing and midwifery, which carry high cognitive demands but offer limited psychological support. The strong association between phone anxiety and higher dependence observed in our study may reflect not only individual vulnerability but also a lack of institutional frameworks that promote healthy digital practices. Furthermore, cultural expectations of constant availability and responsiveness, amplified by peer pressure through messaging platforms and social media, may intensify habitual checking behaviors, including nighttime phone use.
Compared to Western European countries, where digital literacy and digital hygiene are increasingly integrated into university life, Albanian institutions may still lag in incorporating such preventive strategies into their curricula. This absence of formal education on balanced technology use may further explain why emotional and habitual dependence, rather than physical strain, emerged as the dominant dimension of smartphone use in our findings.
These cultural and institutional gaps highlight the need for context-specific interventions. Addressing smartphone addiction in Albania may require more than raising awareness; it may necessitate systemic changes in how universities support student well-being, facilitate engagement beyond the screen, and promote a balanced academic lifestyle.
This study has some limitations that should be considered when interpreting the results. First, the sample was limited to students from a single university, which may reduce the generalizability of the findings to other student populations in Albania or beyond. Second, data collection relied on self-reported questionnaires, which can introduce bias due to social desirability or inaccurate recall. Third, the cross-sectional design restricts our ability to infer causal relationships between smartphone use and dependence. Lastly, some relevant factors, such as mental health status or academic performance, were not assessed, which could confound the observed associations. Future studies should consider longitudinal designs, broader samples, and incorporate objective measures to better understand smartphone addiction dynamics.
CONCLUSION
This study examined smartphone usage and dependence among university students in Shkodra, revealing a growing emotional and behavioral attachment to smartphones. A significant proportion of students reported prolonged daily use (approximately six hours), suggesting a heightened risk of developing addiction-like behaviors. Emotional distress when separated from devices, reported by 84.6% of participants, underscores the psychological toll of excessive use.
The findings align with global concerns, indicating that smartphone addiction is particularly prevalent in university environments, where young adults heavily rely on digital devices for academic and social interaction. Physical symptoms, such as neck and wrist pain, reported by 23% of students, highlight the somatic impact of sustained usage.
These results underscore the urgent need for universities to implement awareness campaigns and structured interventions promoting healthy digital habits. Educational programs should focus on screen-time management, regular breaks, and balanced technology use.
Future research should explore longitudinal outcomes and test the effectiveness of targeted prevention strategies aimed at mitigating smartphone addiction while supporting academic success and student well-being.
RECOMMENDATIONS
The future recommendations are as follows:
1. Universities should conduct awareness campaigns about the risks of excessive smartphone use and its impact on physical and mental health.
2. They should organize workshops to educate students on healthy smartphone usage, including tips for managing screen time and reducing dependency.
3. They should establish counseling services to help students struggling with smartphone addiction and offer guidance on managing digital habits.
4. They should encourage students to take regular breaks from their phones, especially during study sessions, to improve focus and reduce physical strain.
5. Universities can create guidelines for responsible smartphone use, especially during classes and academic activities, to help students maintain balance.
6. They should also encourage students to engage in physical activities that reduce the negative effects of long smartphone usage, such as stretching or exercise breaks.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: Z.S.H., E.H.: Study conception and design; E.P., A.G.: Data collection; Z.S.H., E.H.: Data analysis or interpretation; Z.S.H., E.H.: Methodology; E.P., A.G.: Investigation; Z.S.H., E.H.: Draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| OLS | = Ordinary Least Squares |
| EFA | = Exploratory Factor Analysis |
| SD | = Standard Deviation |
| SPSS | = Statistical Package for the Social Sciences |
| M | = Mean |
| SE | = Standard Error |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for this study was reviewed and granted by the Ethics Committee of the Faculty of Natural Sciences, Department of Clinical Subjects, University of Shkodra (Protocol No. 51/2, dated 12/01/2025, Shkodër, Albania).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this article are available upon reasonable request from the corresponding author [Z.S].
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to the University of Shkodra “Luigj Gurakuqi” for its support and to all participants who provided their opinions regarding the subject.

