All published articles of this journal are available on ScienceDirect.

Stakeholders’ Perceptions of Health Risk Behaviour Engagement among Grades 4-7 Learners in South Africa
Abstract
Background
Health Risk Behaviour (HRB) is an ever-growing concern globally, as well as in countries like South Africa, because of its contribution to disease incidence and premature death. This study explored the perceptions of HRB engagement among Grades 4-7 learners and key stakeholders in Paarl, South Africa, to inform the development of an evidence-based behavioural modification programme.
Methods
A qualitative, exploratory design was employed, and data were collected from school principals, nurses, and learners through seven semi-structured interviews conducted between October 2021 and July 2022. An inductive thematic analysis identified key HRBs, including substance use, bullying, and early sexual curiosity, as well as the environmental influences of family dysfunction, community violence, and gang culture.
Results
Six major themes emerged, highlighting the multifaceted nature of HRB and the need for targeted interventions. Results suggest that stakeholders perceive a critical need for programmes incorporating parental education, school-based mental health support, and community-driven initiatives, such as after-school activities, to address these behaviours.
Conclusion
These findings contribute to the theoretical underpinnings of intervention mapping and emphasise the importance of engaging stakeholders in designing culturally relevant and context-specific prevention strategies.
1. INTRODUCTION
The impact of health risk behaviour (HRB) engagement is well documented globally and in South Africa [1-3]. It is recognised that the incidence of HRB is not waning amongst adolescents, and change is needed regarding behavioural choices that place these individuals at risk of substance abuse, feeling unsafe, unsafe sexual practices and the risk of trauma. The link between risky behavioural choices and their significant contribution to disease incidence and premature death should not be ignored [4].
Despite many programmes targeting a variety of HRB interventions [5-7], successful reduction in HRB engagement is slow, with prevalence figures in South Africa remaining high among youth and adolescents. A study by Visser et al. (2003) noted that 14% of primary school learners used alcohol, and 4% used marijuana. More recently, Daniels et al. (2023) found that in grade 4-7 learners, 36.3% of boys and 28.3% of girls had smoked cigarettes, and 28.7% of boys and 23.8% of girls consumed alcohol without permission, while approximately 17% of boys reported having smoked marijuana in primary schools in South Africa [8, 9]. More alarmingly, the realisation that adolescence may be too late to effectively change risky behavioural choices may be vital in unlocking the next step in behavioural modification programmes.
Decision-making in youth is complex, and facilitating behavioural modification requires a multifaceted approach [7]. However, for modifiable behavioural outcomes to be achieved, the creation of health promotion programmes typically involves the review of pertinent literature, gathering new data, and engaging with experts, community members, and stakeholders in the planning phases [10]. It is also pertinent that this data is grounded in relevant behavioural theories that best represent the community the programme intends to target. Therefore, engaging with learners and other stakeholders in the community when building an HRB prevention programme is vital in the clinical research process as it promotes inclusion and partnerships with individuals exploring their unique perspectives [11].
This thematic analysis aimed to explore the perceptions of learners in grades 4 through 7 and other influential stakeholders on HRB engagement, influences on risky behavioural choices, and possible solutions to include in a prevention programme in the Paarl community of the Western Cape, South Africa. This study is the third data collection phase in a series of studies utilising the intervention mapping framework for health promotion programme design. Intervention mapping (IM) is a framework for theory- and evidence-based health promotion planning grounded in community-based participatory research to ensure that the intervention matches priority population needs and context [10].
2. METHODOLOGY
This study forms part of the primary investigators’ (KD) doctoral study in building an HRB prevention programme targeting grades 4 to 7 learners in South Africa, utilising an intervention mapping framework.
2.1. Study Design
A qualitative, explorative study design was employed to explore stakeholders’ perceptions regarding HRB engagement among grades 4 to 7 learners. Stakeholders who agreed to participate included school principals, nurses from local clinics, and learners in grades 4 to 7, covering individual and organisational input and peri-urban and rural settings. Inductive thematic analysis allowed for a comprehensive analysis of the stakeholders' exposure, experiences and perceptions of HRB to inform the planning of an evidence-based behaviour modification programme.
2.2. Study Setting
The study was conducted in Paarl in the Western Cape, South Africa. It included two principals (from peri-urban and rural) schools, two nurses (from peri-urban and rural) clinics and learners from four schools (three from peri-urban and one from rural). Paarl is a peri-urban area in the Western Cape, South Africa (approximately 60km from the city centre), characterised by socioeconomic challenges, including high poverty levels, substance abuse, and exposure to violence. These factors significantly influence health risk behaviours (HRBs) among youth.
2.3. Sampling
Purposive sampling was used to select learners in grades 4 through 7 and influential stakeholders based on their knowledge, interaction with learners, and role in the community.
Stakeholders invited to participate were school principals/teachers, nurses at primary care clinics, and police officers. Due to COVID-19 restrictions and logistics, the police officer could not participate in the study, and only two of the four school principals could participate. Interviews had to be modified according to the convenience of the stakeholders.
2.4. Sample Size of Learner Focus Groups
In the case of phenomenological research, it was estimated that five learners per grade repeated at the four primary schools would suffice if the interviews produced enough in-depth data to ensure the objectives of the study were reached and recruit enough participants that would lead to data saturation (a point where ‘no new information added is expected to enhance or change the findings of the study’ [12]).
2.5. Procedure
Following ethical approval, seven semi-structured, focused group and individual interviews were conducted between October 2021 and July 2022, following strict COVID-19 sanitation and distancing rules. Due to logistical issues during data collection, principal interviews were conducted individually and face-to-face. Two researchers were present at each interview (KD and HP), one to facilitate questioning and one to move between spaced-out individuals (COVID-19 regulations) to ensure the quality of the recording.
2.6. Data Analysis
An inductive approach was used to generate innovative ideas. An interview guide comprising open-ended questions was developed based on the larger study's original objectives and the thematic analysis's aim. Questions explored the stakeholders' understanding of HRB, exposure to HRB, perceptions of the causes of risky behaviour engagement, and suggestions for future programme planning. Interview questions covered multiple HRBs. Twenty learner volunteers were selected from each of the four schools (5 students per grade; Grades 4-7). Interviews were conducted in English or Afrikaans, depending on the stakeholder’s comfort level. Initial questions were followed up with probing questions for clarification purposes. Each interview lasted between 35 and 45 minutes. The audio recordings were translated and transcribed verbatim using Cockatoo software™ and verified for accuracy by the primary researcher (KD) and moderator (HP). Where possible, transcriptions were forwarded to stakeholders as a form of member checking to ensure the transparency and validity of the transcription.
2.7. Coding
A reflexive, inductive thematic analysis informed by Braun and Clarke’s (2021) six-phase analysis (i.e. 1. Fimiliarization; 2. Generating initial codes; 3. Generating themes; 4. Reviewing potential themes; 5. Defining and naming themes; 6. Producing the report) was conducted [13]. Data were read and re-read to familiarise the primary researcher (KD) and the moderator (HP) with the content. Open coding was used to identify new and emerging codes and categories. After a comparison of the codes and categories, a joint codebook was created. KD and HP refined the initial coding into separate recurring themes for trustworthiness, and after an iterative debriefing process, the final codes and themes were added to the codebook. Transcript thematic analysis was performed using NVivo 14 software.
2.8. Ethical Considerations
Ethical clearance was granted from the Research Ethics Committees and Higher Degrees Committees of the University of Kwa-Zulu Natal (HSSREC/00001649/2020). Permission to conduct the study was obtained from the Western Cape Education Department, principals, and governing bodies of the schools involved. The participants were informed throughout the research that their participation was voluntary and that they could choose not to participate or withdraw at any given time during the study without any consequences.
Learners were provided with a detailed explanation of the research before completing the questionnaire and subsequent interviews. Confidentiality and anonymity were assured to those learners who participated. All precautions concerning COVID-19 safety and prevention of infection will be followed.
3. RESULTS
The demographic profile of the participants is presented in Table 1. Table 2 highlights the HRB perceptions of the stakeholders. Stakeholder perspectives were explored under three categories, according to the study's aims (i.e. Engagement, Influence and Solutions), where six main themes emerged.
| Name | Age Group Classification | Total [n=84] | Gender | Type of Interview | Setting |
|---|---|---|---|---|---|
| Nurse 1 | 51 - 60 | n=1 | Female | Focus Group | Peri-Urban |
| Nurse 2 | 51 - 60 | n=1 | Female | Focus Group | Rural |
| Principal 1 | 51 - 60 | n=1 | Male | Individual | Peri-Urban |
| Principal 2 | 41 - 50 | n=1 | Male | Individual | Rural |
| School 1 | 9 - 14 | n=20 [5 learners per grade] |
Male and Female | Focus Group | Rural |
| School 2 | 9 - 14 | n=20 [5 learners per grade] |
Male and Female | Focus Group | Peri-Urban |
| School 3 | 9 - 14 | n=20 [5 learners per grade] |
Male and Female | Focus Group | Peri-Urban |
| School 4 | 9 - 14 | n=20 [5 learners per grade] |
Male and Female | Focus Group | Peri-Urban |
| Theme | Sub-Theme | Verbatim Quotes |
|---|---|---|
| Category 1: Engagement | ||
| Understanding Health Risk Behaviour |
“Sweet food. Yes, like you have the wrong food.” School 1 “To drink alcohol at a young age.” School 1 “Dagga rook [Grade 5]” School 2 “Tik [methamphetamine] [Grade 7]” School 2 “Buttons [mandrax] [Grade 5]” School 2 “Cigarettes [Grade 7]” School 2 “I understand that there is a trend towards children who have enough exercises, who have enough food or proper food sources in their body, to function, to think, especially at school, in the case of the brain is the food that you eat.” Principal 1 |
|
| Cause and Effect |
“If you start experimenting with alcohol and smoking and using a weapon, being abusive—all those things come from seeing certain behaviours at home.” Nurse 1 “Maybe because they live in certain areas, they don't get the proper nutrition.” Principal 2 |
|
| Curious Minds, Risky Finds | Alcohol Use |
“Yes, I have seen my friend drinking alcohol.” School 1 “They drink wine, kraan,’ and beer.” School 2 |
| Smoking |
“Dagga rook.” Learner, Grade 5, School 2 “They smoke ma skelm... that's how it is from those kids.” Principal 1 “I mean, the grades four to seven they prone to smoking a lot, but the boys are fighting and drinking.” Nurses 1 |
|
| Sexual Curiosity |
“Because they want to be in a relationship... because they just want to kiss and kiss.” School 3 “There are some of our girls; there are some of our kids who are active. I know because I ask them if they use any injections or pills, and there are those that talk.” Principal 1 |
|
| The Fight for Survival | Fighting [Bullying] |
“Someone fights you in the school; there is a school next to our clinic, and teachers will bring children down... in intervals, they start fights with weapons.” Nurse 1 “They are being bullied. [Grade 6]” School 2 “Because there are skollies [hoodlums] at school, they feel unsafe at school.” School 2 “Because they are afraid that their enemies will attack them at school.” School 2 “When a teacher hits you. When you are in a big class.” School 4 |
| Category 2 Influence | ||
| The Smoke and Mirror Effect | Community and Gang Influence |
“Maybe poverty plays a role. It is part of the cycle of life. If you have enough exercises that you get, it has an effect on your movement” Principal 1 “I would say it's the behaviour of the learners or children or people that influences. Down to the influence that they have in their communities, like for instance using drugs or making the wrong choices that influences their health negatively.” Principle 2 “They run around with 'pangas' and chase us.” School 1 “They are gangsters... they stab with knives. Yes, we see it every day.” School 2 “Yes, sir. They shoot a lot.” School 3 “At school, boys will either use pens or come with sharp weapons to defend themselves.” Nurse 1 “Children on the farms are being used by older guys... cannabis is being sold by the children in that age group.” Nurse 2 |
| Peer Pressure |
“The children are sent home or their parents called because they tried some dagga at school.” Nurse 1 “Because they are circled out [Separated/Isolated]” School 3 “By older children that are bigger than them” School 3 |
|
| Substance Normalisation |
“If a child is raised in a household where alcohol use and smoking is a daily norm, then for that child, it's normal to do that.” Nurse 2 “Their mother gives them money, and then they buy the coals. The parents give them the money to buy it, and then they do it in front of the parents.” School 1 “And sometimes they see the parents drinking, and then they take of that.” School 2 “They see it in the house. Their parents smoke and drink.” School 3 “Sometimes, parents and teachers don’t really see it as a health risk. So, children don’t realise it either.” Nurse 2 “I would say mostly at home. Because that is where we see everything, we hear everything, and for the parents and the community, it's become a norm. They don't see it as a health risk behaviour, so the child is seeing this also as a norm, so they mimic the norm all throughout their life, and sometimes they never realise what is the norm.” Nurse 2 |
|
| Breaking the Chain | Home Environment |
“It's not just the man beating the woman. It's also the mother beating the father.” Learner, School 4 “They start at home, they did not get their way, and then they go to school, or they are just triggered with one thing, and then the fight starts.” Principal 1 “But if you look at them, you see how they have grown up. The mother is already dead, the father is already dead, or the mother can't raise them anymore, and they stay with the grandmother or the auntie.” Principal 1 “I think they see the fighting at home and weapons to them; I think it’s a norm. When they do fight over weekends on the farms, there are weapons involved” Nurse 1 “Mainly a lack of a father figure” Principal 2 |
| Role Modelling |
“The children see parents fighting and think it’s a norm to solve problems this way.” Nurse 1 “Parents give their kids money to buy cigarettes, and they smoke with them. It's normal.” School 2 “I can say it easily: 60% of the children in our school are very hard-hearted. The fact that they don't have their own biological parents. So, they stay with their grandparents or people that have adopted them, and that's where the problems come in.” Principal 1 |
|
| Role of Parents |
“They are allowed certain behaviours, to be the big man at home... we have parents that are too young or grandparents raising children that are too tired to discipline a child.” Nurse 2 “There's nobody at home giving them positive reinforcement.” Nurse 2 “And if you look at the parents also, the children that we have the problems with, intellectually, the parent left school by grade 6, grade 5, and they think that it's supposed to be like that, and she's being abused, so they also think that maybe it should be like this. At least he can defend himself, you know what I mean?” Nurse 2 “They see it in the house. Their parents smoke and drink.” School 3 “Their mother gives them money and then they buy the coals. The parents give them the money to buy it, and then they do it in front of the parents.” School 1 |
|
|
Category 3 Solutions |
||
| Momentum for Change | Suggestions for future programmes |
“To get the adults involved in the child’s education. Teach them some skills other than the normal work that they do on the farm, labourers and so on. The program can help them [Parents] to build the relationship with their children.” Principal 2 “Parenting skills, how to discipline a child and how to nurture your child from the newborn age, how to nurture a child they don't know how to do it, they don't talk to their children, they really don't talk to a child I'm talking about the newborn now, I look at them, and I think, don't you cuddle this child and nurture the child when we give an injection, for example, they like robots.” Nurse 2 “Yeah. Talks involving the police, and we do it now. We involve the police to have more talks about drug abuse and alcohol abuse and not just that, abuse towards older people at home.” Nurse 1 “There must not be gangsters. They must take them away. They must live somewhere else.” “There must not be any drugs. Drugs must not exist.”. “They must stop shooting, sir.”. “They must partake in activities, sir, like sports. And artwork” School 1 “We must get the children off the streets and take the alcohol away. And to help them to stop bullies.”. “To walk to church.” School 3 |
4. DISCUSSION
This thematic analysis explored the perceptions of different stakeholders, including grades 4-7 learners. It provides a more in-depth understanding of risky behaviours that the learners engage in or are exposed to in various environments. The most concerning prevalent HRBs, as identified by the stakeholders, included alcohol use and smoking, particularly among boys; bullying and fighting, predominantly in the school environment; sexual curiosity and experimentation at an early age; and gangsterism. All these factors could significantly influence risky behavioural choices.
4.1. Category 1: Engagement
4.1.1. Understanding Health Risk Behaviour
The understanding of HRB varied considerably amongst the stakeholders. The learners were most direct, stating what they considered to be risky behaviours. Younger learners (grade 4) identified sweets and food that are “bad” for you as their understanding of risky behaviour. In contrast, older learners (grades 5 and 7) had a more pragmatic view and identified alcohol, smoking and drugs as HRB. The principles viewed poverty and poor nutrition as possible contributors to poor decision making and risky behavioural choices. The nurses had a more cause-and-effect view, identifying experimentation and carrying weapons as precursors for HRB engagement. The Centre for Disease Control defines HRB as “actions or patterns of activity undertaken by individuals that increase their likelihood of negative health outcomes, such as chronic disease, injury, or premature death. These behaviours typically include physical inactivity, poor dietary habits, substance abuse, unsafe sexual practices, and behaviours that contribute to unintentional injuries or violence.” [14]. It would thus appear that each stakeholder had a piece of the larger picture when understanding HRB; however, their perspective is limited by their occupational role or direct experiences [in the case of the learners], preventing them from seeing the bigger picture.
4.1.2. Curious Minds, Risky Finds
Alcohol use, smoking and sexual curiosity were among the most prevalent HRBs identified by the stakeholders. Visser et al. (2003) and Daniels et al. (2023) are the only known studies looking at primary school learners in South Africa. Alarmingly, over the last 20 years, not only were similar HRBs identified by learners, but the significant rise in the prevalence indicates that South Africa is on a negative trajectory in the fight against HRB prevention [8, 9].
Puberty is a challenging time for both parents and teens alike. It is associated with a need to express strong personal values and explore their limits and abilities. It is also characterised by youth taking more significant risks than adults [15] and justifying their risk by weighing up the pros and cons of the risk and the social norms around which behaviours are acceptable [16]. Sexual curiosity was identified by principals, with reports of learners being sexually active and knowledgeable about contraceptives. A study by Attila et al. [2022] found a significant positive association between sexual curiosity and sexual behaviour among adolescents in Ghana [17]. Mallanzi et al. (2023) identify that for a young adolescent to make good choices about their sexual behaviour, a coherent and positive sense of self-identity is key [18]. Once again, the concept of self-identifying during the pre-adolescent age is pivotal in informing choices to engage in behaviour that is deemed risky. Extrinsic factors such as poor parenting, drug use, peer pressure, sociocultural standards, mass media and individual attitudes are all occasionally associated with risky behavioural choices and engagement [18]. Thus, teens could interpret these risky behaviours as “thrill seeking” and associate it with positive risk behaviour as it is the accepted “norm”.
4.1.3. The Fight for Survival
Bullying and physical fights are prevalent in the school environment, with both nurses and principals identifying boys as particularly prone to these behaviours. Overcrowded classrooms, where survival and dominance are essential to social standing, contribute to the problem. This is consistent with a South African study by Mguye (2024), which identifies overcrowded conditions and inadequate resources as catalysts for aggressive behaviours [19]. Often, fighting originates out of the need for a sense of belonging. Learners want to perform, impress, show off and assert dominance in an overcrowded school setting. A study by Brooks et al. (2012) emphasised that a sense of belonging within a neighbourhood, a solid connection to school and active parental involvement in decision-making were linked to a lower likelihood of HRB engagement. Conversely, a weaker sense of family belonging and low connectedness to teachers was associated with higher engagement in multiple risky behaviours [20].
Bullying has been linked to violent behaviour, substance abuse and poor academic outcomes [21]. Bradshaw et al. 2013 suggest a conceptual and potentially etiological overlap between bullying and risky behaviours such as engaging in violence, gang membership and carrying a weapon. Furthermore, both bullies and bully-victims may be attracted to gangs and carry weapons as a means of protection, particularly in the urban context [21].
4.2. Category 2: Influence
The influence category looked at the environments the learners are exposed to and the impact on their well-being. The category featured sub-themes such as the home environment, role modelling, the role of parents, peer pressure, substance normalisation and community and gang influence. The themes are explored collectively, highlighting their interconnectedness and impact on various subsystems.
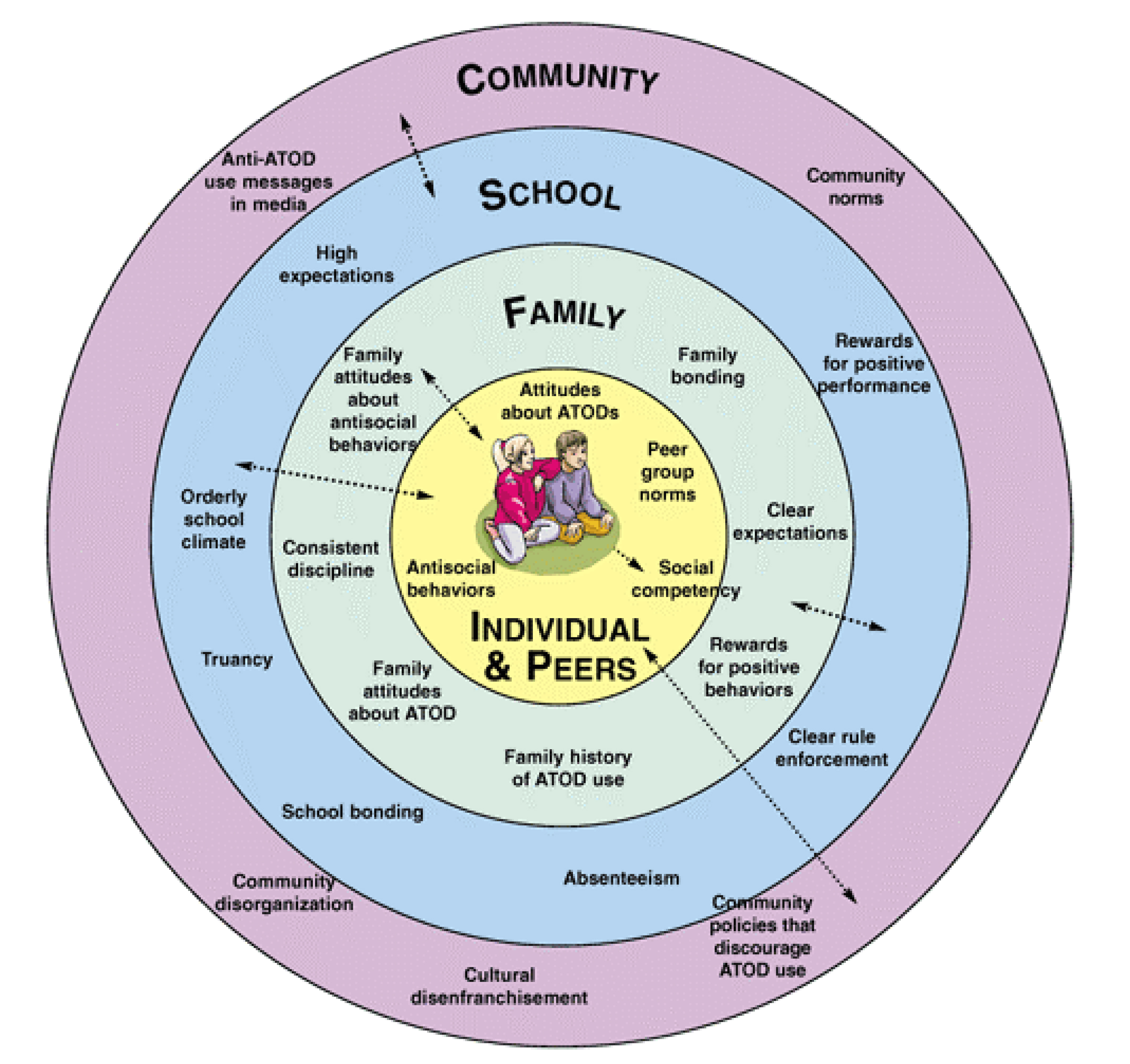
The relationship between the environment and its impact on behavioural choices can best be understood through Bronfenbrenner’s ecological theory. Bronfenbrenner highlighted the crucial role that social environments play in a child's upbringing, identifying the disintegration of family structures as a primary factor behind the rising levels of alienation, apathy, rebellion, delinquency, and violence among American youth [22].
4.2.1. Breaking the Chain
The home and school environments, central to the learner's individual microsystem (immediate environments), are the places all stakeholders frequently reported as the breakdown point. All stakeholders reported behaviours and activities in the home environment that are carried over to other environments such as school. Structural breakdown within the home environment reported included: Lack of a father figure, neglect, poor role modelling, substance use such as alcohol consumption and smoking in front of the learners, which normalises the behaviour, parents sending the learners to buy cigarettes thus interaction within the community and parents not identifying the behaviour as a health risk and not having the basic skills required for effective parenting. Maphaphuli (2023) explains that children who are exposed to constant conflict, aggression, abuse, neglect, domestic violence and separation because of divorce or parents who work long hours away from home are likely to present with behavioural and emotional problems [23]. Life in a family with dysfunctional dynamics is a turbulence of uncertainty and instability characterised by conflicts between parents, tense relationships, chaos, neglect, abuse, poor communication, lack of empathy and secrecy to the extent that the emotional and physical needs of the family members are not met, especially children [23].
The ecological theory suggests that this level of uncertainty and insecurity means that children looking for affirmations that should be present in the child/parent relationships seek attention elsewhere, usually in inappropriate places [24]. Both nurses and principals highlight the lack of parenting skills and stability within the home environment, and this filters through to the school environment, leading to learners engaging in smoking and violent behaviour.
4.2.2. The Smoke and Mirror Effect
Learners were aware of the adverse effects of gangsterism and the toll it takes on their mental well-being. Learners reported that they wanted gangsters “thrown in jail” and that the police should “shoot them dead” or that they should “shoot each other dead”. While learners are aware of this influence at a community level, according to the nurses, gangsters target vulnerable children in the community and “groom them” from a young age. For the easily influenced or vulnerable child, gangs could offer a sense of belonging, self-identity, protection, a distraction from a dysfunctional home and a solution to the poverty at home. The origin of gangs within the poverty-stricken, low-income areas of Cape Town (known as the Cape Flats) has its roots in community service and protection that the then-Apartheid government would not provide the communities. These communities were often displaced from land considered to be of more value from various parts of Cape Town and thrown together in one area. Thus, the gangs protected their communities and patrolled their territory, keeping outsiders from entering. However, the merger of the gang scene and prison scene saw the introduction of drugs and gun trades within communities. The protection of territory soon became the protection of economically viable trade deals, only benefitting gang bosses and usually at the detriment of the community. While most adults in the community condemn the violence and drug dealing of the gangs, they do see gangs as protection. This conflicting view has normalised gangsterism and provided children with easy access and limited options.
4.3. Category 3: Solutions
4.3.1. Momentum for change
The final goal of this thematic analysis was to explore, from stakeholders, possible solutions for inclusion in a HRB prevention programme. This may be the most crucial goal as it ensures that a future prevention programme is adaptable for the intended community. Intervention programmes often fail due to a lack of participation from the intended target audience and the stakeholders immediately around them [25]. Thus, it was imperative to gain the perspectives of the learners, as this evokes a bottom-up approach and ensures programme buy-in [10]. The cultural context of a prevention programme is of critical importance as this reveals the extent to which the programme can be implemented with fidelity [26].
Once again, the learner's perspectives were more direct, emphasising the removal of drugs, alcohol and gangsters. While this perspective is easier said than done, an interesting comment emerged; “We must get the children off the streets”. This speaks to the need to occupy children's free time after school. Suggestions from the nurses and principals focussed on parent skill development and engaging with the police and other community stakeholders to build better communication networks within the community. A summary of the key suggestions to include in a prevention programme targeting grade 4-7 learners is listed below:
• Parental involvement and education, addressing the need for parenting skills and stronger family relationships.
• Community engagement, offering alternatives to gang involvement and substance abuse through organised activities such as sports or community-based programs.
• School-based interventions focus on reducing bullying, providing mental health support, and fostering a safe environment.
CONCLUSION
This thematic analysis reiterates that contextual factors such as family, school and community have a massive influence on the lives and behavioural choices of grades 4-7 learners in the Paarl community, Western Cape, South Africa. Alcohol use, smoking, bullying, and gangsterism are prevalent, often rooted in the unstable family dynamics and disadvantaged communities where these children live. A holistic approach involving parents, schools, and community leaders is crucial for reducing engagement in risky behaviours. Effective intervention programs should focus on skills development, education, positive role models, and safe home and school environments.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: KJD is the primary author responsible for the overall conceptualisation, article writing and thematic analysis in partial fulfilment of a PhD degree. NC is a project supervisor responsible for conceptualising, thematically analysing, and approving the article. HP is the overall supervisor responsible for the study concept design, thematic analysis and approval of the final article submission. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| HRB | = Health risk behaviour |
| IM | = Intervention mapping |
| COVID-19 | = Coronavirus disease of 2019 |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical clearance was granted by the Research Ethics Committees and Higher Degrees Committees of the University of Kwa-Zulu Natal, South Africa (HSSREC/00001649/2020).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
This project was financially supported by the National Research Foundation (NRF) of South Africa (Thuthuka TK200327510674). The funders had no role in the study design and will not have any role during the execution, analysis, interpretation of results or the decision to submit results.
ACKNOWLEDGEMENTS
Declared none.

