All published articles of this journal are available on ScienceDirect.

A Systematic Review of the Rate of Attainment in Controlling Non-communicable Diseases (NCDs) in the Eastern Mediterranean Region (EMR)
Authors Info & Affiliations
Abstract
Introduction
The overall causality of modern public health, especially in the field covered by the Eastern Mediterranean Region (EMR), can be attributed to the Non-Communicable Diseases (NCDs). The review lists the adopted strategies, compares the successful and failed cases, and outlines the endemic setbacks to achieving global agenda progress.
Methods
Based on PRISMA, a literature search was conducted to identify articles published between January 2010 and December 2024 across PubMed, Scopus, Web of Science, and Google Scholar. The studies that would have met the eligibility criteria are those concerning the WHO-specific categories of the NCDs and their risk determinants or interventions to control the disease as part of the EMR jurisdictions.
Results
There was a total of fifty studies that met the inclusion criteria. Countries that had strong national action plans, that is, Turkey, the United Arab Emirates, and Qatar, were observed to bear significant similarity in WHO goals, particularly in tobacco prevention and screening measures. Contrary to that, in Cairo (Egypt) and Baghdad (Iraq), NCD mortality was still high (76 and 78.4, respectively). Kuwait (37.8%) and Qatar (36.5) had the highest levels of obesity, and Saudi Arabia had the highest levels of diabetes prevalence (15.3).
Discussion
Though implementation of policy directives has spread throughout the EMR, they are not strictly enforced or maintained.
Conclusion
Though there is gradual progress, EMR countries are still vastly below the WHO vision of 2025 to see a 25 per cent reduction of premature deaths due to NCDs. To mobilise effective action, the synthesis of country-specific and measurable evidence is of paramount importance.
1. INTRODUCTION
Non-Communicable Diseases (NCDs) are those diseases that have been named by the World Health Organization (WHO) and considered to be chronic and which cannot be passed through humans or which are not acute in nature. They can continue for a very long period of time and in a very slight process. The leading ones are cardiovascular diseases, diabetes, chronic respiratory ailments, and cancers [1, 2]. Although they overlook mental health conditions, injuries, and road-traffic accidents, the academic and policy discourses that are situated in differing health agendas, NCDs are now the greatest burden of infection, with over 70 per cent of global deaths attributed to the condition [1]. The prevalence of NCDs is also high in the Eastern Mediterranean Region (EMR), which is a 22-country region in diverse socioeconomic and cultural milieus, leading to approximately 75 per cent of all deaths in many of the member states [1, 3]. The multifactorial nature of the increased pace of NCDs in this geopolitical territory can be profounded at the following points: rapid urbanisation, the increased consumption of energy-dense, nutrient-poor diets high in sugars and fats, sedentary lifestyles associated with technological advances, and the widespread use of tobacco products [4]. Following the introduction of the Global Action Plan for the Prevention and Control of NCDs 2013-2025, an agenda that stipulates the use of tangible targets in the reduction of untimely deaths caused by the four lead NCDs by 25 percent by 2025, the region has been focusing on such a low-carbon mitigation strategy in four prongs. This plan aims at reducing exposure to key risk factors, that is, tobacco use, poor dietary habits, lack of exercise, and dangerous drinking habits; furthermore, enhancing health systems to identify and deal with the illness at an early stage [5]. At the same time, there are multiple states within EMR that promulgated national frameworks to address the NCDs. These policy action plans have institutionalised tobacco control laws, encouraged physical exercise, introduced healthier eating habits that are healthier, increased clinical quality of early diagnosis and continuous management, and staged campaigns on awareness to the population, among other things [6, 7]. However, significant implementation challenges remain. They include insufficient healthcare systems, lack of medical expertise and training, ineffective funds towards the provision of healthcare to the masses, and unequal provision of care to the diverse population groups [8, 9].
Empirical evidence shows that NCD surveillance has not been adequate in most low- and middle-income countries, despite the increasing morbidity and socio-economic consequences of these diseases [10, 11]. Although developed countries have a higher relative burden of NCDs, the absolute burden is highest in middle-income countries when population size is taken into account [12, 13]. This review, hence, aims at questioning the current situation of the NCD control campaigns in EMR countries by analysing the achievements in relation to WHO targets. It will list the effective interventions that are implemented in different national settings and highlight the unending challenges that hinder the proper management of NCDs. With the understanding of the complexities of the dynamics of NCDs in the context of EMR, the stakeholders will be able to redefine strategic interventions to accommodate the urgent health needs and protect the sustainability of the public-health programmes on a long-term basis. The current assessment critically evaluates the rate of achieving WHO NCD goals by state EMRs, distinguishing between successful approaches to the issue and current obstacles to direct other, more effective and sustained regional actions.
2. MATERIALS AND METHODS
2.1. Methodology of the Review
This systematic review was conducted within the framework of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [14], and all the PRISMA checklist items were adhered to. The protocol of reviewing was developed before the start of the study, and all the procedures were taken in relation to the well-established guidelines on systematic reviews.
2.2. Design of the Research Question
The study question has been framed based on the PICO framework [15]. Such a framework answered this as it enabled the clear definition of the population, intervention/exposure, comparison, and insights of interest. To be used in this review, the following was the specification of the components: Population (P): Populations living in countries of the Eastern Mediterranean Region (EMR) of the World Health Organization. Intervention / Exposure (I): National strategies, policies, or programmes meant to intervene upon Non-Communicable Diseases (NCDs) and their major risk factors. Comparison (C): International differences in prevention and control measures of NCDs adoption, implementation, and effectiveness. Outcome (O): Development toward the WHO Global Action Plan 2013–2025 goals of NCDs, including reduced mortality, prevalence of primary risk factors (tobacco use, obesity, diabetes), and activities in the responsive health-system.
2.3. Search Strategy
To find the necessary information, an extensive literature review of publications from the past 14 years (January 2010-December 2024) was conducted. It was conducted through a systematic and multifaceted analysis of four electronic databases: PubMed, Scopus, Web of Science, and Google Scholar. The search approach combined controlled vocabulary and free-text concepts related to NCDs and EMR states, such as those that include phrases like non-communicable diseases, cardiovascular disease, cancer, diabetes, chronic respiratory disease, and names of the countries used as constituents. These terms were optimally combined using the operators of Boolean (AND, OR). All citations were retrieved through EndNote 20(r) [16], then duplicates were eliminated. Relevance screening of titles and abstracts was done independently by two reviewers, and subsequently, a full-text screening of potentially eligible studies at two instances was done with respect to preset eligibility criteria. Any discrepancy during both screening levels was overcome by voting or seeking a third opinion from the reviewer.
2.4. Inclusion and Exclusion Criteria
Suitably qualified research studies were those that focused on NCDs as defined by the World Health Organization (i.e., cardiovascular diseases, diabetes, cancers, and chronic respiratory diseases). Prevalence, risk factors, national/regional approaches, or general public health policies of EMR countries (according to the WHO classification of 22 EMR states). Provides original empirical information (quantitative or qualitative) or an assessment of interventions/programmes. Two reviewers conducted data extraction using a standardised form and recorded the following: (i) research characteristics (author, year, country, design), (ii) characteristics of the population, (iii) type of NCD or risk factor, (iv) policies or interventions appraised, and (v) outcomes with references to the WHO global targets in NCD. Research papers were filtered out if they were conducted at medical centers with other medical issues not classified as NCDs by WHO (e.g., mental health, injuries, road traffic accidents). Reflective commentaries, editorials, conference abstracts, or any other non–peer-reviewed material lacked sufficient methodological detail or did not meet baseline quality standards.
2.5. Quality Assessment
Design-appropriate appraisal instruments, Cochrane Risk of Bias Tool (randomised controlled trials) and Newcastle- Ottawa Scale (observational studies) were used to assess the quality of methodology of the included studies. Ratings of the studies were done based on the adequacy of the sample, rigour in methodology, statistical analysis, and clarity in reporting.
2.6. Data Analysis
Thematic analysis was used to qualitatively analyse the data. The findings were categorised into key domains, which were policy development, risk factors control, healthcare integration, public awareness campaigns, and barriers to its implementation. The heterogeneity of the study designs and outcomes made it impossible to conduct a meta -analysis. Instead, the use of descriptive statistics and narrative synthesis was to summarise the achievement of progress towards the WHO global NCD targets in EMR countries. The standardisation of progress was based on a transparent, uniform rubric aligned with the WHO Global NCD Action Plan 2013 -2025. The first goal is a relative decrease of 25% of the premature deaths (ages 30–70) between 2010 as the baseline and 2025 due to the four major NCDs. Secondary targets are at least a 10% relative decrease in harmful use of alcohol, at least a 10 percent relative decrease in physical inactivity, at least a 30 percent relative decrease in tobacco use, at least a 25 percent relative decrease in elevated blood pressure, and termination of the increase in the incidence of diabetes and obesity. To provide uniformity, the progress of each country was placed into three categories: High (97 percent above target), moderate (34 percent to 97 percent above target), and low (33 percent and below target). All prevalence and mortality rates were age-adjusted to the WHO World Standard Population to ensure fair cross-country comparisons. Data sources were mostly of three types: the WHO Global Health Observatory, which provided 2020 estimates of 15 countries; national WHO STEPS surveys of 2016 to 2020, which were used when 3 or more national data points were unavailable, and where 3 or more regional weighted-average imputation (used in 4 countries) [17-21].
3. RESULTS
3.1. Search Results
A comprehensive search of a plethora of databases produced 3, 240 records in the first place. After eliminating 2780 duplicates in EndNote [16], there were 460 articles left. The abstracts were further screened, and 215 records were eliminated in the process. A thorough review of the whole text of the 245 articles saw 195 articles being dropped on the basis that they did not match the objectives of the study. As a result, 50 articles were included in the review (Fig. 1).
3.2. Advancement in Policy Formulation
Some of the EMR countries have realised impressive progress in the development and enforcement of their national policies. There is an example of high-performance in Turkey, Qatar, and the United Arab Emirates, having an extensive plan of national action, a solid tobacco control law, and implemented NCD services in the health system. Conversely, Egypt, Lebanon, and Iraq are characterised by low levels of policy development, largely due to political instability and weak implementation capacity.
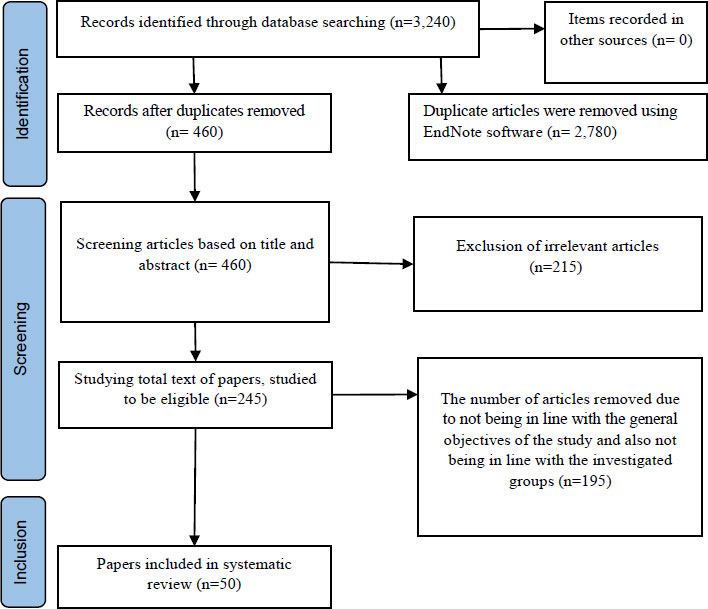
The process of searching and screening selected articles based on PRISMA guidelines.
3.3. Community Sensitization and Prevention Programs
The promotion of the implementation of the practice of public health has been well embraced, though with inconsistent vigor. Countries with high income, including Qatar, the UAE, and Saudi Arabia, have developed widespread campaigns on diet and physical activity at the national level, whereas school-based and community-based interventions are more common in middle- and low-income countries. Data show that population-wide campaigns are more effective at creating awareness, but in situations with limited resources, sustainability becomes problematic.
3.4. Healthcare Systems Penetration
The integration of the management of NCD into primary healthcare has been sporadic. In Lebanon, Iran, and Jordan, screening programmes of hypertension and diabetes have been in place, but due to resource limitation scale up has not been achieved. On the other hand, Turkey and the UAE have been found to take a systematic approach in incorporating NCD care as a component of health services, including the early detection programmes and training of primary healthcare workers.
3.5. Analysis of WHO- Standardised Indicators (Comparison between Countries) (2010-2020)
There is still a rate of more than 70 per cent when it comes to NCD mortality in most of the countries, with high rates in Egypt (76 per cent) and Iraq (78.4 per cent), indicating diminished progress. The highest levels of obesity exist in high-income Gulf countries, such as Kuwait (37.8%), Qatar (36.5%), and so on, because of sedentary lifestyles. The prevalence of tobacco use is a particular case with Turkey (28 0) having the highest prevalence rate despite the strong regulatory interventions and Iran (13.6 0) having a lower prevalence rate. In Saudi Arabia (15.3%) and Turkey (12%), the prevalence rates of diabetes are significantly high, which is in line with poor dieting habits and lack of exercise. High fasting plasma glucose and hypertension are ubiquitous in all environments, and this highlights the dual nature of the problem of obesity and metabolic risks.
3.6. Key Findings
The synthesis of the cross-country comparisons based on the WHO statistics and studies done by peers provides the following insights: Countries that have been developing national action plans and surveillance mechanisms have made more progress in terms of NCD goals. It is the high-income nations that have a disproportionate burden of obesity and diabetes, even though they have more resources. The major obstacles in the low-performing countries are represented by the political crisis and weak health systems. Table 1 presents the standardised data about the chosen countries and includes the policy interventions, policy outcomes, and prevalence rates.
| Country | Progress Toward NCD Targets | Key Interventions Implemented | Challenges Faced | NCD Mortality Rate (%) | Obesity Prevalence (%) | Tobacco Use (%) | Physical Inactivity (%) | Diabetes Prevalence (%) | Hypertension Prevalence (%) | High Fasting Plasma Glucose (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Iran | Moderate | National action plan for NCDs; integration into primary healthcare; public awareness campaigns; screening programs for diabetes/hypertension | Data gaps; disparities in healthcare access | 72.4 | 27.8 | 13.6 | 52.0 | 9.4 | 21.1 | 15.0 |
| Turkey | High | Comprehensive tobacco control laws; nutritional guidelines; health promotion campaigns targeting physical activity; national dietary guidelines | Cultural resistance to lifestyle changes | 73.0 | 32.1 | 28.0 | 38.0 | 12.0 | 30.5 | 16.3 |
| Jordan | Moderate | National strategy for NCDs; routine screening programs for diabetes/hypertension; health education initiatives; community health worker programs | Limited resources in rural areas; high unemployment rates affect access | 74.5 | 29.4 | 22.0 | 60.0 | 10.5 | 24.0 | 14.8 |
| Saudi Arabia | Moderate | “Healthy Lifestyle” campaign; school-based programs; periodic screening for adults; initiatives to reduce salt intake | High prevalence among youth; cultural norms around diet/exercise | 75.2 | 35.0 | 12.0 | 67.0 | 15.3 | 27.5 | 18.2 |
| Egypt | Low | School programs promoting physical activity, public awareness campaigns on healthy eating, and limited access to diabetes management services | Political instability affecting delivery; lack of funding | 76.0 | 34.6 | 15.0 | 61.0 | – | – | – |
| United Arab Emirates | High | National school canteen guidelines; integration into national health strategies; extensive screening programs | Variability across emirates; reliance on expatriate labor with varying literacy | 71.5 | 27.9 | 19.0 | – | – | – | – |
| Oman | Moderate | National screening program for citizens aged ≥40 years; campaigns on healthy lifestyles, including nutrition/exercise | Resource limitations in rural settings; need for more trained personnel | 70.8 | 24.5 | 10.5 | – | – | – | – |
| Lebanon | Low | Screening initiatives for high-risk populations; public awareness campaigns on risk factors | Ongoing political/economic crises affecting systems | 77.1 | 29.7 | 23.0 | – | – | – | – |
| Iraq | Low | Limited campaigns focused on improving primary healthcare services post-conflict | Ongoing conflict affecting access/delivery | 78.4 | 30.5 | 20.0 | – | – | – | – |
| Bahrain | Moderate | Health promotion initiatives targeting obesity/diabetes prevention; community engagement focused on nutrition education | Cultural attitudes towards diet/exercise may hinder progress | 72.8 | 27.0 | 15.6 | – | – | – | – |
| Qatar | High | Comprehensive policies focusing on nutrition/physical activity; national screening programs for early detection | Rapid lifestyle changes leading to increased obesity rates among youth | 68.9 | 36.5 | 14.9 | – | – | – | – |
| Kuwait | Moderate | Public health campaigns addressing obesity/diabetes prevention including school-based education/community fitness events | High prevalence of sedentary lifestyles among youth | 75.4 | 37.8 | 18.7 | – | – | – | – |
4. DISCUSSION
The results of this systematic review highlight the significant progress made by those countries in the Eastern Mediterranean Region (EMR) in their efforts to address Non-Communicable Diseases (NCDs) and the unresolved issues that hinder the appointment of effective disease control in contributing to a successful solution. Three to four years of country-level data synthesised between 2010 and 2020 make this review define not just the policy adoption but also the progress and gaps that can be identified in terms of the major WHO indicators. Due to the rising popularity of NCDs, understanding the implications of these findings takes center stage in the eyes of policymakers, health practitioners, and the general population who are determined to improve health outcomes in the region. The creation of the national action plans and policies that address the NCDs is one of the critical developments in the EMR. Countries like Iran and Turkey have developed strong structures that follow the WHO guidelines, and therefore, portray practical interest to address the rising burden of NCDs. As an example, the high prevalence of tobacco in Turkey has fallen sharply due to the comprehensive tobacco control measures, and this demonstrates the extent to which stringent legislation can lead to positive health effects as a result [22]. The Iranian provincial data, based on twelve years of WHO data, showed that the prevalence of cigarette-smoking among the population dropped significantly; the 2005 statistics stood at approximately 14.65 per cent, whereas in 2016, the prevalence of smoking had decreased significantly to about 10.63 per cent (a drop to 10.63 per cent) [23]. However, in spite of the recorded improvements, there are high rates at which the effectiveness of such policies depends on their execution and enforcement [7]. Political will is critical in many situations, where laws are made and followed. The political instability or conflict faced by countries, e.g., Lebanon and Iraq, is a major hindrance to the implementation of health policies. This variance can be seen in Table 1, whereby the prevalence of the use of tobacco in Lebanon reaches above 40% and is in conspicuous contrast to the slowly decreasing trend in more established environments [24]. These statistics underscore the need to have a sustained political will and system of governance that gives high priority to the health programs despite other socio-political issues that cross the board [8, 25-27].
Public-awareness campaigns have been a useful tool for educating the populations on the risk factors of NCDs and healthier lifestyles. The Saudi Arabian and Lebanese campaigns can be viewed as examples of the possible influence of the targeted communication strategy on changing behaviour. However, to attain success in these endeavours, they have to be culturally sensitive and highly customised to local beliefs and practices. As an illustration, although the benefits of encouraging exercise are universal, approaches towards encouraging exercise can vary significantly depending on cultural perspectives of exercise and leisure. The recent evidence of high prevalence of obesity within the Eastern Mediterranean Region, with prevalence levels exceeding 40 whilst in Qatar they remain high, highlights the fact that structural measures are necessary to stem this vice beyond the witnessing of awareness campaigns [28, 29]. The relevance and effectiveness of health-promotion campaigns can be increased significantly when the local communities are engaged in the planning and execution of the campaign. In addition, social media platforms are also a strategic avenue of targeting younger populations who would be more vulnerable to digital communication [30, 32]. Inclusion of NCD in the primary healthcare system is essential in the provision of timely screening, diagnosis, and treatment. Our results suggest that such nations as Jordan have achieved significant advancement in this area due to regular screening of high-risk groups. However, there are still major problems with hospital capacity and its access. The healthcare systems in most of the EMR countries are not well-funded, especially in rural areas, where accessibility to healthcare services is still a problem. There is therefore a need to strengthen the primary healthcare infrastructure in a bid to enable early detection and proper management of NCDs. This involves investing in health care centers, improving health care training programs by the health care workers, and ensuring there are the required drugs. Moreover, the quality of care offered to NCD patients may be improved if a patient-centred approach is adopted. This model focuses on holistic management that takes into account patients' physical, emotional, and social needs and ultimately achieves high health outcomes [33-35]. The disproportionate development facilitation observed in Table 1, like the more successful cases of hypertension identification in Jordan relative to Sudan, depicts the effects of dissimilar primary-disparate care integration in the area [36, 37].
The continuing predicaments of NCDs management in the EMR include the weakness of the healthcare system, lack of data, socioeconomic inequalities, and cultural obstacles, which require an all-encompassing, evidence-based, and multi-faceted strategy towards the effective prevention and management of the condition. Improving healthcare systems is paramount, and it requires significant investments in infrastructure to enhance service provision, such as renovating medical institutions, providing necessary diagnostic devices, and generally increasing access to specialist services for NCDs. At the same time, today clinical competencies and patient outcomes can be enhanced with the help of continuous professional development, learning in the form of simulations, making the provision of training programmes to healthcare professionals, in particular, nurses, more effective, which the existing research confirms by confirming the effects of workforce capacity building [38, 39]. Strong data-collection methods are also essential and require that they have common, interoperable data-gathering systems that can track the trends and risk factors of NCDs as well as the results of their intervention. These systems ought to be in line with WHO guidelines in ensuring that there is consistency and comparability across EMR countries [40, 41]. As we review, the countries that have well-established surveillance networks, e.g., Qatar and the UAE, always have complete trend information on obesity and hypertension. However, in weak states such as Sudan and Yemen, the gap in the available data prevents proper monitoring and hinders effective interventions that can be used by the government and the population in fighting diseases [11, 42]. Socioeconomic inequality is a crucial factor in the healthcare accessibility of all groups, and intervening to provide remedies to this issue through policies like subsidies of care among low-income earners, mobile medical services to rural communities, and social protection interventions to alleviate the financial burden is highly recommended, as demonstrated by effective models in resource-limited environments [43, 44]. In addition, the culturally sensitive interventions by the government in the field of health should be implemented in terms of specific collaboration with the community leaders and the stakeholders to develop the programmes that would respect the beliefs and traditions of the community and practices, resulting in the increase of the level of campaign acceptance and efficacy as the example of the community-based health-promotion activities demonstrates [45]. Such results emphasize the fact that popular, one grounds fit all strategies are not applicable to the region. Multi-sectoral approaches are essential in long-term NCD management in the EMR through multi-sectoral collaboration with the government, healthcare providers, and civil society.
To realize the WHO's aspiration of a 25 per cent reduction in premature mortality from non-communicable diseases by 2025, the nation's EMR users are invited to adopt available initiatives whilst addressing deeply rooted inhibitions with solid, evidence-based approaches. Future directions should focus on strengthening multisectoral cooperation and integrating disciplines such as education, agriculture, and urban development to create conditions conducive to healthy living and thereby align with WHO-based integrated NCD prevention models [46]. As seen in the reviewed literature, the EMR states with active multisectoral programmes, such as the case of the Healthy Cities Initiative in Iran, have a better fit with the WHO goals to address the non-communicable disease compared to those that mostly rely on health-sector interventions [47, 48]. The need to promote research and innovation should remain central, and there should be a focus on developing context-specific interventions, including digital health methods, of which such approaches as telemedicine and mobile health apps have proven effective and can be implemented in resource-limited environments [49, 50]. Increasing the involvedness of the community with participatory, community-based interventions has the potential of promoting ownership and driving towards sustainable behaviour change, as demonstrated with successful health promotion initiatives in a wide cultural milieu [51].
5. LIMITATIONS
There are a number of constraints that surround this review. The presented studies showed the heterogeneity in terms of design, sample size, and the quality of methodology, thus limiting the generalisability of results. In addition, disparate quality, the assessment tool was used in the appraisal of observational studies and randomised controlled trials, which may have introduced a flaw of variance in evidence assessment. The age, sex, and economic disparities among studies could bring about nonapplicability across the heterogeneous EMR countries. Large gaps in data, especially in the low- and middle-income states, hindered the proper estimation of NCD prevalence, risk factors, and the results of interventions. The lack of cross-country comparability and tracking of the achievement of WHO targets is smothered by the absence of standardised, cross-country interoperable NCD surveillance systems. The 22 member states of the EMR have divergent socioeconomic, cultural, and political vectors, which could imply a mindless, exhaustive capture of the challenges in conflict-laden regions like Iraq and Lebanon, or in rapidly urbanising regions like Qatar and the UAE. Perceptions of diet, physical exercise, and seeking health care were identified as barriers, but their depth within particular communities may have been under-investigated. The scope of the review, which is confined to English and Arabic literature, exposes validity, as well as there might be some positive publication bias that may exaggerate the perceived intervention efficacy. Limiting the period to 2010-2024 might exclude recent data that could indicate a new policy trend or health outcomes. As the policy uptake is recorded, the long-term sustainability and effectiveness of implementation on the ground are questionable because of the political instability, financial limitations, and instability of the healthcare system. The use of qualitative thematic analysis instead of quantitative meta -analysis limits the accuracy of the estimates of the effectiveness of the intervention or the assessment of trends in NCD. The focus on the non-empirical case, including opinion pieces, expert commentaries, etc., might have left crucial contextual information about the impediments and facilitators of NCD containment in the EMR out. All these restrictions emphasise the need to interpret the results cautiously, and the need to promote better standardisation of surveillance, nation-specific implementation statistics, and strict quantitative analysis measures in further scholarly work.
CONCLUSION
The prevalence of non-communicable conditions in the Eastern Mediterranean Region is a massive public health issue of concern; however, progress has been made through policy development, sensitization programs, and incorporation of NCD into primary care. This review highlights, by synthesising cross-national trends over 2010-2020, the finding that those states, which have a comprehensive national action plan and strong surveillance mechanisms, such as Turkey, Qatar, and the UAE, have achieved more quantifiable progress in achieving the WHO targets on NCDs. Valuable hurdles remain, especially in low and middle-income economies, and they include access to healthcare, political vagaries, and policy implementation inconsistency. Multidimensional, evidence-based interventions, such as primary healthcare infrastructure strengthening, multicultural health promotion, and multisectoral collaboration, to address these dilemmas, will not only be important for controlling NCDs. Clinicians and policymakers are placed at a central position in leading the policy implementation, exploitation of digital health innovations, integration of patient-centred care models, and ensuring even distribution of access to the preventive service. The present review, therefore, highlights the need to institutionalise NCD management as part of primary care, strengthen screening programmes, and gender insensitive approaches towards behavioural and metabolic risk factors. However, the results should be approached with reservations due to the heterogeneity of the studies, the lack of data, and the differences in the health system capacities between the EMR countries. Future studies need to be focused on improving the data collection strategies, investigating the issues of the implementation, and conducting quantitative studies to provide a stronger, country-specific NCD governance evidence.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: S.S., A.R.Y., M.S.G., M.A., A.A.A. and R.R.: Wrote the main manuscript text, while S.D. and K.H.: Were responsible for designing the study and supervision. All authors reviewed and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| NCDs | = Noncommunicable Diseases |
| EMR | = Eastern Mediterranean Region |
| WHO | = World Health Organization |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PICO | = Population, Intervention/Exposure, Comparison, Outcome |
| STEPS | = STEPwise approach to Surveillance (WHO STEPS surveys) |
| RCTs | = Randomized Controlled Trials |
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
ACKNOWLEDGEMENTS
Declared none.

